Schistosomiasis in Tanzania
Schistosomiasis, also known as bilharzia, is a parasitic infection caused by schistosoma parasites that use freshwater snails as an intermediate host. The parasite is transmitted to humans through contact with contaminated freshwater, typically in rural areas with poor sanitation. Schistosomiasis is endemic to regions with freshwater lakes, hydroelectric dams, and extensive agricultural irrigation.
Once inside the human body, the schistosoma parasites can lay eggs that cause inflammation and damage to the organs, including the liver, spleen, kidneys, and bladder. Symptoms of schistosomiasis include abdominal pain, diarrhea, bloody urine, and itchy skin.
Chronic schistosomiasis can lead to severe health problems, including anemia, stunted growth, diminished cognitive function, and increased susceptibility to other infections, including HIV. Of the neglected tropical diseases (NGDs), schistosomiasis is one of the most prevalent with over 200 million people worldwide estimated to be affected and 700 million people living in endemic areas, primarily in sub-Saharan Africa, but also in parts of South America and Asia.
Schistosomiasis risk factors are socio-economic, ecologic, and biologic; therefore, integrated efforts are necessary to control transmission. Communities affected tend to have frequent water contact, which can include fishers, farmers using irrigation sources, people doing household chores using freshwater sources, swimmers, and bathers.
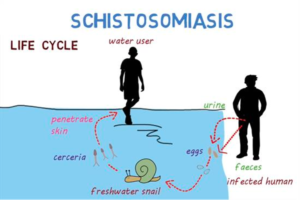
Prevention and control of schistosomiasis involve improving sanitation, providing access to clean water, reducing snail populations, educating populations about risk factors and the nature of the disease, and treating infected individuals with medication, typically the chemotherapy drug Praziquantel. The image below demonstrates the life cycle of the schistosoma parasite.
The Burden in Tanzania and the Rorya District
Schistosomiasis has been studied in Tanzania since the early twentieth century. Ninety percent of schistosomiasis cases globally are in sub-Saharan Africa, and Tanzania has the second highest prevalence after Nigeria. During the 1970s and 80s, Tanzania built new irrigation systems and dams to provide water for agriculture for the growing population. These innovations, however, led to an expansion of schistosomiasis risk areas and the number of people affected. Over half of all Tanzanians live in high exposure regions. In addition, 40% of Tanzanian households lack access to safe drinking water, and 60% lack access to improved sanitation, putting them at high risk for exposure to schistosoma parasites. In 2019, around 15 million people, almost a quarter of the Tanzanian population, required treatment for schistosomiasis.

Schistosomiasis is widespread in the Rorya District, where Maji Safi Group works, as many people use Lake Victoria as a water source for household activities and for bathing. In addition, selling drinking water and fishing are major economic activities in the area. Using netting, traps, and hook and line fishing, fishermen frequently come in direct contact with infected water, and the same is true for their spouses and children who are also involved in the fishing process.
Empowering Communities to Prevent Schistosomiasis
Mass drug administration (MDA) is one of the key interventions recommended by the WHO for prevention and control of neglected tropical diseases (NTDs). In Tanzania, Praziquantel is distributed on a large scale to schools and communities. However, knowledge about the disease and how to prevent or treat it is integral for reducing future cases. Many people still do not have access to treatment, and others prefer not to take the treatment due to a lack of information. This, added to the fact that one can become reinfected, shows why control is difficult using treatment alone. Studies have shown that interventions addressing behavioral and cultural dimensions of transmission are more effective at preventing and controlling schistosomiasis than those that use environmental and treatment interventions alone.

Maji Safi Group‘s Community Health Educator (CHE) model engages communities and facilitates behavioral change by teaching disease prevention and WASH education. Maji Safi Group’s CHEs receive specific training and travel to markets, schools, health care facilities, and fishing communities to teach about occupational hazards as well as causes, prevention, and treatment for waterborne diseases, including schistosomiasis. For over a decade, our full-time cadre of community-based educators have built relationships with Rorya communities and provided a trusted source for information and resources through numerous innovative, community-driven programs. MSG has also been involved in specific projects that addressed schistosomiasis.

2017
In 2017, a group of public health and social work students from the Brown School of Social Work at Washington University in St. Louis came to Shirati to learn about participatory tools alongside MSG’s Community Health Educators. The students and CHEs joined with leaders from the Tanzanian Fisheries Research Institute (TAFIRI) to visit Beach Management Units (BMUs), which are centers where fishermen must officially register in order to legally fish. They used participatory tools within fishing communities to learn about the issues they face around waterborne diseases, including schistosomiasis, and to co-generate solutions to reduce prevalence.

2022
Aligning with UN Sustainability Goals, Maji Safi Group partners with local institutions, like schools and healthcare systems, to promote sustainable health and development. In 2022, we collaborated with the Shirati KMT District Hospital to address schistosomiasis via several health care facilities (HCFs). Doctors and nurses did the testing and provided medication as needed, while Maji Safi Group’s Community Health Educators provided in-person education and distributed leaflets about schistosomiasis. So far, MSG has developed collaborations with seven health care facilities in the Rorya District and has reached close to two thousand people. We continue collaboration with the Shirati KMT District Hospital to monitor the progress and impact of this ongoing intervention.
Measuring Success

From 2015-2019, MSG did over 25,000 health screenings to gauge disease rates in the community and the impact of Maji Safi Group’s WASH education. The testing showed that the prevalence of schistosomiasis in Shirati exceeded the national average. In addition, the results consistently demonstrated high prevalence of schistosomiasis in community members, but also a significant decrease in prevalence among community members who had participated in MSG’s health and disease prevention programs in schools and the community.
Find out more about MSG’s five years of health screening data here.
The Future
While mass drug administration (MDA) has been and continues to be an important part of schistosomiasis control, the nature of the disease, the environmental and occupational aspects of transmission, and the fact that people can become reinfected necessitate the development of more targeted and integrated methods of control. Community engagement, a heavy emphasis on education, and multi-sectoral partnerships can motivate the behavior change, knowledge, and practices that reduce the burden of schistosomiasis in the communities where MSG works. Together with the Tanzanian and local government’s commitment to preventing and controlling schistosomiasis, we can help our partner communities reach their goals of health and well-being and help eliminate the poverty-trap of NTDs like schistosomiasis.
In the future, Maji Safi Group will:
- Continue to acknowledge that locally relevant programs co-created with community input are key to reducing NTDs through community-driven initiatives and close collaboration with health authorities.
- Collaborate with public health researchers at the universities around the world using genomic, epidemiologic, and ecologic factors to understand local ecosystems of infection and how to target prevention and control programs.
- Continue to build WASH Hubs (community centers) where residents in the Rorya District can access clean water and where staff, drawn from the local community, can provide training and support on specific occupational risks and prevention strategies for farmers and their families regarding waterborne disease transmission.
- Seek opportunities to cooperate with educational institutions in Tanzania and globally on schistosomiasis research projects and effective measures for control and prevention in endemic areas.
